Dutta-Bergman, M. (2004). Reaching unhealthy eaters: Applying a strategic approach to media vehicle choice. Health Communication, 16, 493-506.
Dutta-Bergman, M. (2004). An alternative approach to social capital: Exploring the linkage between health consciousness and community participation. Health Communication, 16, 393-409.
Dutta-Bergman, M. (2004). Describing volunteerism: The theory of unified responsibility. Journal of Public Relations Research, 16, 353-369.
Dutta-Bergman, M. (2004). Interpersonal communication after 9/11 via the telephone and the Internet: Theory of channel complementarity. New Media and Society, 6, 661-675.
Dutta-Bergman, M. (2004). Poverty, structural barriers and health: A Santali narrative of health communication. Qualitative Health Research, 14, 1-16.
Dutta-Bergman, M. (2004). The unheard voices of Santalis: Communicating about health from the margins of India. Communication Theory, 14, 237-263.
Dutta-Bergman, M. (2004). Developing a profile of consumer intention to seek out health information beyond the doctor. Health Marketing Quarterly, 21, 91-112.
Dutta-Bergman, M. (2004). Primary sources of health information: Comparison in the domain of health attitudes, health cognitions, and health behaviors. Health Communication, 16, 273-288.
Dutta-Bergman, M. (2004). The impact of completeness and Web use motivation on the credibility of e-Health information. Journal of Communication,54, 253-269.
Dutta-Bergman, M. (2004). Health attitudes, health cognitions and health behaviors among Internet health information seekers: Population-based survey. Journal of Medical Internet Research, 6, e15. Retrieved June 2, 2004, from http://www.jmir.org/2004/2/e15/index.htm
Dutta-Bergman, M. (2004). An alternative approach to entertainment education. Journal of International Communication, 10, 93-107.
Dutta-Bergman, M. (2004). Complementarity in consumption of news types across traditional and new media. Journal of Broadcasting and Electronic Media, 48, 41-60.
Dutta-Bergman, M. (2004). A descriptive narrative of healthy eating: A social marketing approach using psychographics. Health Marketing Quarterly, 20, 81-101.
Foreign migrant workers washing luxury condo in Singapore
Foreign migrant workers painting luxury condo in Singapore
Foreign migrant workers relaxing on their Sunday day off in Singapore
Responding to the continued rise in COVID19 clusters in migrant worker dormitories in Singapore, and building on earlier research (See CARE White paper Issue 6), this White Paper reports on the findings of a survey conducted with low-wage migrant workers in Singapore. In addition to the poor living conditions highlighted earlier, the structural constraints on preventive behavior are explored. Drawing on the key tenets of the culture-centered approach, the research highlights the powerful role of structural factors such as arrangements of dormitories, the absence of hygienic conditions because of the structures, the lack of clean toilets, pressure on limited toilets, and scarcity of water. The findings highlight the challenges to mental health and wellbeing experienced by the workers. Moreover, it points to the absence of voice infrastructures, and the ways in which this absence contributes to conditions that are rife for the pandemic. Solutions for structural solutions and voice democracy are offered.
by Gayle Moana – Johnson, CARE – Community Research Assistant and Mohan J. Dutta, Director,Center for Culture – centered Approach to Research & Evaluation Massey University
In this white paper, the community advisory group in Highbury, working with community researcher Gayle Moana-Johnson, developed the key conceptual guidelines for culture-centered community-grounded testing. The white paper highlights the key concepts anchoring the partnership between the community advisory group and the clinical team at HHPNZ
This white paper outlines the key principles of culture-centered community-led testing that are voiced by the advisory group of community members in Highbury, anchored in the principle of representing the most “in-need” members of the community (referred in the rest of this white paper as the “margins of the margins”). The key ideas in this white paper are developed as anchoring principles for the partnership between the community advisory group and the Health Hub Project New Zealand (HHPNZ).
Communicative leadership is anchored in the idea of communication as community, communication as both the primordial source of community, and communication as a resource in manifesting community. Communication forms the infrastructure of community.
Be it in its local manifestation, in its national articulation of a collective identity, or in its global networks in response to crises, community is built on communication.
Communication as communion brings together participants in spaces, creating the basis of shared values, shared meanings, and shared actions. It is through the fundamental work of communication as bridging, as bringing people together, as creating the basis of dialogue, as creating the framework for forming and sustaining relationships that we come to realize communities.
It shouldn’t take a pandemic to make evident the powerful role of communication as constitutive of community, locally, nationally, and globally. Also, it shouldn’t take a pandemic to recognize the urgency of principled communication, one that is anchored in the search for truth, in transparency, in dialogue, and in democracy.
And yet, we are here.
Globally we are in the midst of a pandemic because of communicative failures at multiple layers of leadership across the globe, from authoritarian regimes that worked hard to hide the initial information about the epidemic, to opaque global institutions that are co-opted by the agendas of authoritarian regimes, to neo-fascist political parties that have taken over some of the world’s largest democracies, driven to power by their manipulative campaigns that thrive on hate and division.
The failure of much of global leadership to respond to the pandemic, to develop preventive resources, to create and sustain health infrastructures, and to care for communities is fundamentally the failure of communication.
Donald Trump, Jair Bolsonaro, Narendra Modi, Boris Johnson, globally we are witnessing the implications of communicative failures across nation states. Each of these men have risen to power through the deployment of communication as an instrument of hate.
Trump draws his power from simplistic narratives of the “outsider threat,” which forms the infrastructure of his “Make America Great Again” campaign. It is no surprise then that he finds refuge in the “Chinese virus,” triggering a wide range of anti-Asian incidents of hate in the U.S.
Modi’s popular appeal thrives on the use of hate to prop up an imaginary of a Hindu India, built precisely through the exclusion of its Muslim other. For a political project that was right until the COVID19 outbreak orchestrating the xenophobic exclusion of India’s Muslims through its National Registry of Citizens, it is no surprise that the COVID19 threat would be catalysed to orchestrate Islamophobia.
Driven by the deployment of communication as propaganda, U.S., Brazil, India, and U.K. have witnessed the pitfalls of communicative failure in the backdrop of COVID19. Communication, in its utter ugliness, thrives on circulating propaganda on one hand. On the other hand, it systematically obfuscates the failure in governance, the absence of basic public health and welfare infrastructures, and the abject failure of the state to care for its poor and underclasses.
In the midst of this evident failure in leadership in some of the largest democracies across the globe, it is humbling to witness a model of communicative leadership in Aotearoa New Zealand that is anchored in care, transparent communication, social justice, and democracy.
The face of the New Zealand response is the Prime Minister, a student and adept practitioner of communication as communion.
From the initial days of the sharing of the state’s COVID19 response to the ongoing lockdown that the country is witnessing, Prime Minister Jacinda Ardern appears on the screen at least once or twice a day. Her daily briefings to the press are fed through a wide range of broadcast and new media. You witness a leader that takes the care to respond to the most difficult of questions, supported by accurate information grounded in scientific knowledge, and sincerely committed to transparency. If there are questions she does not have the information on, she states so openly and with clarity.
Communicative leadership is transparent, this is one of the first lessons we learn from the response in Aotearoa.
Communicative leadership is evident in the clarity and preparation with which the lockdown was implemented in Aotearoa. Each of the different levels of response to COVID19 were explained with clarity, along with the specific behaviors being recommended in each of the levels. The message with the behavioral recommendation was simple and is repeated multiple times across channels. The Minister of Health and the Director General of Health communicated information clearly about the number of cases, the status of the cases, and the steps being taken to “flatten the curve.” A dedicated Government website communicates the information clearly and with daily updates.
In addition to her meetings with the Press, the Prime Minister draws on her highly popular Facebook live platform to participate in conversations. She takes the time to read questions and directly respond to them, often getting online from home in an informal setting.
Her responses are not mediated by public relations teams or crisis consultants.
This is communicative leadership in action, authentic in its dialogic potential. It is this very authenticity that forms the basis of community, a key part of the Prime Minister’s ongoing message to New Zealanders, to do what New Zealanders do best: respond to COVID19 as a community, caring for each other, and taking care of each other.
Care also forms the basis of a strategy that incrementally moved into the lockdown. An initial level 3 alert gave people an opportunity to prepare, before the level 4 lockdown was implemented. During this period, there was ample communication about the evidence driving the decisions, the basis of the decisions, the explanations for the behaviors being recommended, and the support available to enable the behavior.
Care and social justice form the basis of the Labour-led response strategy in Aotearoa. The lockdown has been supported with state-driven financial support for employees, with paid leave support given to organizations to ensure job security. Similarly, policies have targeted rents to be paid during the lockdown. The Minister of Finance often accompanies the Prime Minister in communicating the financial policies being put into place for support. Anchoring these policies in justice ensures that the rights of workers and low-income communities are at the forefront of the conversation.
The strong presence of Māori culture in Aotearoa shapes the state’s response to kaumātua (the aging members of communities) with care, ensuring their wellbeing is placed at the heart of the response. Communities across Aotearoa reflect this communicative leadership in local spaces, responding with mutual aid and support for each other. Communities of care anchored in mutuality hold up communicative leadership.
That robust democracies are integral to COVID19 response means that there ought to be ample room for plural voices, for questions to be raised, and for evidence to be shared based on experiences in communities to shape a climate of dialogue. In our work at the Center for Culture-centered Approach to Research and Evaluation (CARE) in Aotearoa, this opening for ongoing dialogue based on community voice is perhaps one of the strongest elements of communicative leadership. Even as we develop advocacy papers based on questions emerging from communities, we often find that the issues we raise have already been addressed at a rapid pace.
Democracies depend on their abilities to listen to the people that own them. We witness in the COVID19 response in Aotearoa this accountability to the people, supporting a flexible infrastructure that is continually responsive to the pandemic and its changing nature.
Certainly there are ongoing challenges as the state responds to the changing numbers and scale of the pandemic. A communicative leadership has the robust capability to respond to these ongoing challenges because it is based on the recognition of the fundamental role of communication in making our communities and in sustaining them.
In an earlier OpEd, I wrote about COVID19 offering us a window into imagining new ways of organizing our communities, democracies, and the earth. Communicative leadership is a key ingredient in this work of imagination.
“It takes a pandemic to render visible the deep inequalities that make up the highly unequal societies we inhabit. As pandemics go, the power of COVID19 lies in its mobility, along the circuits of global capital, picked up and carried by the upwardly mobile classes feeding the financial and technology hubs of capital.
The irony of neoliberal globalization lies in the disproportionate burden of accelerated mobilities borne by the bodies of the poor at the global margins. The poor, whose bodies are the sites of neoliberal extraction, are also the bodies to be easily discarded when crises hit.
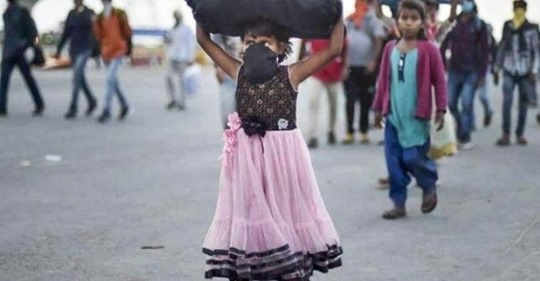
The images of throngs of people, the poor, now expelled from their spaces of precarious work at the metropolitan centers of financial and technology capital, spaces that are projected as the poster-models of mobility in development propaganda, walking on the long walk home, are circulating across our mobile screens.
Images of a migrant worker dead after the gruelling walk home, a mother pulling her daughter as they try to make their way home, a young man bursting into tears at the sight of food, a father walking as he carries his sleeping daughter on his shoulders, crowds of workers waiting in long lines to board buses, these are the faces of the unequal India made visible by COVID19.
These images of emaciated men and women, with little children, carrying pots, torn down bags and dilapidated beddings on their heads, walking on the roads and highways that form the infrastructures of the new India are haunting reminders of the masses of displaced people expelled by wars, riots, genocides, and famines.”
Mohan J. Dutta Director, Center for Culture-centered Approach to Research & Evaluation, Massey University
Foreign migrant workers washing luxury condo in Singapore
Foreign migrant workers painting luxury condo in Singapore
Foreign migrant workers relaxing on their Sunday day off in Singapore
Responding to the continued rise in COVID19 clusters in migrant worker dormitories in Singapore, and building on earlier research (See CARE White paper Issue 6), this White Paper reports on the findings of a survey conducted with low-wage migrant workers in Singapore. In addition to the poor living conditions highlighted earlier, the structural constraints on preventive behavior are explored. Drawing on the key tenets of the culture-centered approach, the research highlights the powerful role of structural factors such as arrangements of dormitories, the absence of hygienic conditions because of the structures, the lack of clean toilets, pressure on limited toilets, and scarcity of water. The findings highlight the challenges to mental health and wellbeing experienced by the workers. Moreover, it points to the absence of voice infrastructures, and the ways in which this absence contributes to conditions that are rife for the pandemic. Solutions for structural solutions and voice democracy are offered.
Gayle Moana – Johnson, CARE – Community Research Assistant and Mohan J. Dutta, Director,Center for Culture – centered Approach to Research & Evaluation Massey University
In this white paper, the community advisory group in Highbury, working with community researcher Gayle Moana-Johnson, developed the key conceptual guidelines for culture-centered community-grounded testing. The white paper highlights the key concepts anchoring the partnership between the community advisory group and the clinical team at HHPNZ
This white paper outlines the key principles of culture-centered community-led testing that are voiced by the advisory group of community members in Highbury, anchored in the principle of representing the most “in-need” members of the community (referred in the rest of this white paper as the “margins of the margins”). The key ideas in this white paper are developed as anchoring principles for the partnership between the community advisory group and the Health Hub Project New Zealand (HHPNZ).
Courtesy Julio Etchart as part of CARE’s “Respect Migrant Rights” campaign in Singapore
This white paper responds to the high prevalence of COVID-19 in clusters associated with dormitories that house low-wage migrant workers in Singapore. Based on an ongoing digital ethnography (45 hours of participant observation) conducted in spaces where low-wage migrant workers participate online, 43 interviews conducted between April 7 2020 and April 13, 2020, inputs from advisory group of lowwage migrant workers, and drawing on 157 in-depth interviews conducted since 2013, the following key challenges with housing and food, as well as corresponding key solutions are proposed. Each of the key challenges is presented, alongside specific recommendations for solutions. The participants for the interviews were identified using snowball sampling. The interviews were conducted in Bengali, mix of Bengali and English, or English, depending on the level of comfort of the participant. Given the sense of anxiety expressed by the participants (see theme 7 below), the white paper does not disclose the locations. Also, it does not separate the different forms of arrangements to protect the confidentiality of the participants. The excerpts from the interviews are truncated to protect the identity of the participants. One of the limitations of the current study is the small sample size of the COVID19- specific data gathered between the April 7 and April 13 timeframe; however, the depth of the narratives offer rich contextually-embedded insights into the challenges being experienced by low-wage migrant workers and the potential insights they envision. The CARE research team is currently conducting a follow-up quantitative study exploring everyday experiences of health and wellbeing among low-wage migrant workers.
The findings reported here are drawn from our advisory group of community members that represent the community in Highbury. The advisory group has been built on the basis of purposive sampling, ensuring that the voices of the “margins of the margins” are represented. The advisory group meets face-to-face as well as on a digital platform. The group is facilitated by two community researchers, recruited from within the advisory group and trained in the fundamentals of interview-based research.
A wide range of models have been proposed as frameworks for responding to Covid-19. These models highlight the significance of health communication in preventing the spread of COVID19 as well as in effectively responding to it. The positioning of specific models as solutions to COVID-19 is tied to the creation of actual strategies of response globally. One such model that has been rapidly disseminated in policy discourse and circulated in articulations of COVID response is the “Singapore Model.” Drawing on the key tenets of the CCA, this paper will examine the premise of the “Singapore Model” as a framework for global health.
The white paper draws on the key tenets of the CCA to examine Singapore’s pandemic response. The CCA foregrounds the interplays of culture, structure, and agency in the constructions of health meanings and the development of health solutions.
Structure refers to the political economy of organizing resources in society. Culture reflects the community norms, community-based meanings, and community values guiding relational negotiations of health and wellbeing. Agency reflects the relational and collective capacities of communities to develop solutions.
The global nodes of spread of Covid-19 highlight the significance of health communication in preventing the spread as well as in effectively responding to it. On January 30, 2020, the World Health Organization (WHO) declared the outbreak as a Public Health Emergency of International Concern. Noting the aggressive movement of the virus across countries, with eight countries reporting more than 1000 cases of COVID-19, the WHO declared COVID-19 as a pandemic. Drawing on critical analyses of the pandemic and crises response literatures as well as building on the experiences of CARE in developing culture-centered community grounded interventions,this white paper outlines the culture-centered approach to pandemic response, specifically directed at offering culturecentered guidelines for effective communication. The culture-centered approach foregrounds the interplays of culture, structure, and agency in the constructions of health meanings and the development of health solutions
Dr Phoebe Elers, Dr Steve Elers and Professor Mohan Dutta
This study explores the challenges experienced by residents in Glen Innes, Auckland. The findings have assisted in the identification of local problems and corresponding solutions, including the ‘Poverty is Not Our Future’ campaign, which has served as anchor for residents to challenge dominant structures and, at the same time, communicate their everyday realities of poverty. While this study is focused on Glen Innes, material hardship continues to be a significant issue in Aotearoa New Zealand, with research determining that 13 percent of children lived in households that experienced material hardship in the 2017/18 financial year (Statistics New Zealand, 2019) and that children born into disadvantage in Aotearoa New Zealand have a significant likelihood of remaining disadvantaged (New Zealand Treasury, 2016a, 2016b; Templeton, 2016).
Jolovan Wham is a Singaporean of ethnic Chinese descent. He has been involved in human rights activism, working primarily on issues relating to migrants, the death penalty, and freedom of expression.
He was executive director of Humanitarian Organisation for Migration Economics (HOME), an NGO which provides shelter, education opportunities and legal aid for low waged migrant workers.
He is a member of the Community Action Network, a coalition of activists which promotes civil and political rights. He obtained his bachelor’s degree in social work from the National University of Singapore. His activism has resulted in him being banned by the education minister from speaking at education institutions and campuses.
He will be presenting a Public Talk, Workshop & will be collaborating with Prof. Mohan Dutta,Director,- CARE at Massey University on the topic “Communicative strategies for resisting authoritarianism”.
Date & Time: Wednesday, 27th November @ 12:00 – 1:00 pm
Venue: Palmerston North City Library, Events Centre, Ground Floor, Palmerston North.
Public Talk Abstract:
Authoritarianism is said to be on the rise and democracy in retreat in many parts of the world. Commentators often point out this trend in long standing liberal democracies like the United States but also to the consolidation of power in regimes like China and Russia. What can we learn from Singapore’s experience to combat the rise of authoritarianism? In this talk, Mr Wham will talk about one party rule in Singapore, how it is perpetuated and the State’s and Singapore society’s response to activism and advocacy.
CARE Workshop – Dissent and resistance: Negotiating boundaries in Singaporean activism by Mr. Jolovan Wham
Date & Time: Thursday, 28th November @ 12:00-1:00 pm
Venue: GLB3.02 Manawatu, Massey University
Topic: A free workshop on Dissent and resistance: Negotiating boundaries in Singaporean activism by Mr. Jolovan Wham.
Workshop Abstract:
Activists in one party states or dictatorships are often detained and imprisoned for years. In some cases, they are murdered and disappeared. The Singapore state eschews such extreme tactics and yet retains almost absolute control over the population. What are the opportunities for dissent and resistance in such a controlled environment? What tactics and strategies have activists used to achieve their goals?
Come and hear our speakers launch the CARE White Paper & hear them talk abouttheir white paper on
“Communicative strategies for resisting authoritarianism”
Speaker’s Bio:
Jolovan Wham: is a Singaporean of ethnic Chinese descent. He has been involved in human rights activism, working primarily on issues relating to migrants, the death penalty, and freedom of expression. He was executive director of Humanitarian Organisation for Migration Economics (HOME), an NGO which provides shelter, education opportunities and legal aid for low waged migrant workers. He is a member of the Community Action Network, a coalition of activists which promotes civil and political rights. He obtained his bachelor’s degree in social work from the National University of Singapore. His activism has resulted in him being banned by the education minister from speaking at education institutions and campuses.
Mohan J Dutta: is Dean’s Chair Professor of Communication. He is the Director of the Center for Culture-Centered Approach to Research and Evaluation (CARE), developing culturally-centered, community-based projects of social change, advocacy, and activism that articulate health as a human right. Mohan Dutta’s research examines the role of advocacy and activism in challenging marginalizing structures, the relationship between poverty and health, political economy of global health policies, the mobilization of cultural tropes for the justification of neo-colonial health development projects, and the ways in which participatory culture-centered processes and strategies of radical democracy serve as axes of global social change.